The Department of Health and Human Services’ Office for Civil Rights has published its 2016-2017 HIPAA Audits Industry Report, highlighting areas where HIPAA-covered entities and their business associates are complying or failing to comply with the requirements of the Health Insurance Portability and Accountability Act.
The Health Information Technology for Economic and Clinical Health (HITECH) Act requires the HHS to conduct periodic audits of HIPAA covered entities and business associates to assess compliance with the HIPAA Rules. Between 2016 and 2017, the HHS conducted its second phase of compliance audits on 166 covered entities and 41 business associates to assess compliance with certain provisions of the HIPAA Privacy, Security, and Breach Notification Rules.
The 2016/2017 HIPAA compliance audits were conducted on a geographically representative, broad cross-section of covered entities and business associates and consisted of desk audits – remote reviews of HIPAA documentation – rather than on-site audits. All entities have since been notified of the findings of their individual audits.
The 2016-2017 HIPAA Audits Industry Report details the overall findings of the audits, including key aspects of HIPAA compliance that are proving problematic for covered entities and business associates.
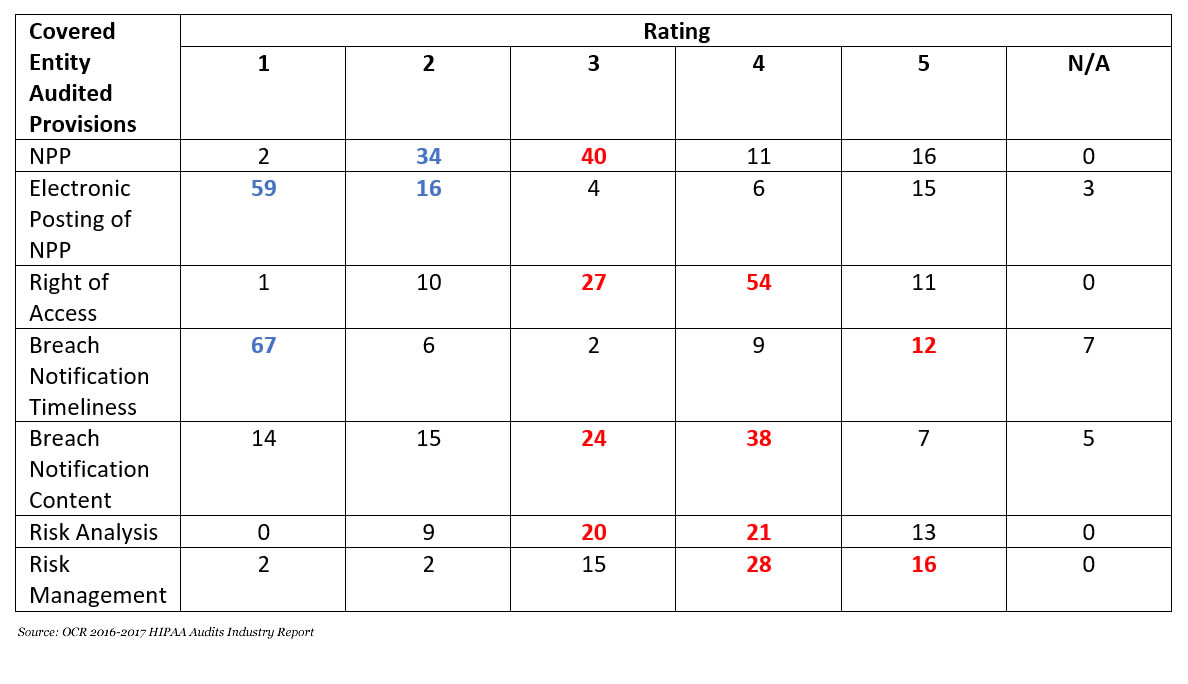
In the report, OCR gives each audited entity a rating based on their level of compliance with each specific provision of the HIPAA Rules under assessment. A rating of 1 indicates the covered entity or business associate was fully compliant with the goals and objectives of the selected standards and implementation specifications. A rating of 2 means the entity substantially met the criteria and maintained adequate policies and procedures and could supply documentation or other evidence of compliance.
A rating of 3 means the entity minimally addressed the audited requirements and had made some attempt to comply, although had failed to comply fully or had misunderstood the HIPAA requirements. A rating of 4 means the entity made negligible efforts to comply, such as supplying policies and procedures for review that were copied directly from an association template or providing poor or generic documentation as evidence of training. A rating of 5 means OCR was not provided with evidence of a serious attempt to comply with the HIPAA Rules.
The table below summarizes the audit results on key provisions of the HIPAA Rules. The blue and red figures indicate the most common rating in each category, with blue corresponding to mostly ratings of 1 or 2 (compliant) and red indicating implementation was inadequate, negligible, or absent.
The table clearly shows that most audited entities largely failed to successfully implement the HIPAA Rules requirements.
 Most covered entities complied with the requirement of the Breach Notification Rule to send timely notifications in the event of a data breach. HIPAA requires those notifications to be sent within 60 days of the discovery of a data breach; however, most covered entities failed to include all the required information in their breach notifications.The audits revealed widespread compliance with the requirement to create and prominently post a Notice of Privacy Practices on their website. The Notice of Privacy Practices gives a clear, user friendly explanation of individuals’ rights with respect to their personal health information and details the organization’s privacy practices. However, most audited entities failed to include all the required content in their Notice of Privacy Practices.
Most covered entities complied with the requirement of the Breach Notification Rule to send timely notifications in the event of a data breach. HIPAA requires those notifications to be sent within 60 days of the discovery of a data breach; however, most covered entities failed to include all the required information in their breach notifications.The audits revealed widespread compliance with the requirement to create and prominently post a Notice of Privacy Practices on their website. The Notice of Privacy Practices gives a clear, user friendly explanation of individuals’ rights with respect to their personal health information and details the organization’s privacy practices. However, most audited entities failed to include all the required content in their Notice of Privacy Practices.
The individual right of access is an important provision of the HIPAA Privacy Rule. Individuals have the right to obtain and inspect their health information. Most covered entities failed to properly implement the requirements of the HIPAA Right of Access, which includes providing access to or a copy of the PHI held within 30 days of receiving a request and only charging a reasonable cost-based fee for access.
The first phase of HIPAA compliance audits conducted by OCR in 2012 revealed widespread noncompliance with the requirement to conduct a comprehensive, organization-wide risk analysis to identify vulnerabilities and risks to the confidentiality, integrity, and availability of protected health information. In its enforcement activities over the past 11 years, a risk analysis failure is the most commonly cited HIPAA violation.
HIPAA covered entities are still failing in this important provision of the HIPAA Security Rule, with the latest round of audits revealing most audited entities failed to implement the HIPAA Security Rule requirements for risk analysis and risk management.
“The audit results confirm the wisdom of OCR’s increased enforcement focus on hacking and OCR’s Right of Access initiative,” said OCR Director Roger Severino. “We will continue our HIPAA enforcement initiatives until health care entities get serious about identifying security risks to health information in their custody and fulfilling their duty to provide patients with timely and reasonable, cost-based access to their medical records.”
You can view the full 2016-2017 HIPAA Audits Industry Report on this link: https://www.hhs.gov/sites/default/files/hipaa-audits-industry-report.pdf.
The post OCR HIPAA Audits Industry Report Identifies Common Areas of Noncompliance with the HIPAA Rules appeared first on HIPAA Journal.