Article Contents
If you own a small practice, here is what to focus on when it comes to HIPAA:
- The owner remains legally responsible.
- A breach costs more than the fine.
- Start with a Security Risk Analysis.
- Maintain policies, training, and sanctions.
- Obtain required vendor agreements.
- Keep evidence of compliance.
- Track federal and state changes.
Small Practice Owner’s Legal Responsibility for HIPAA Compliance
A small practice owner carries legal responsibility for HIPAA compliance regardless of who performs the day-to-day compliance tasks. That means confirming the practice has completed a recent risk analysis, written policies actually reflect what HIPAA requires, staff training stays documented, and HIPAA agreements are in place with every vendor handling patient data. Ownership of a HIPAA-covered practice creates direct financial and legal exposure to fines, corrective action plans, and civil litigation.
Why Ownership Carries the Responsibility
The Office for Civil Rights holds the business liable for a HIPAA violation, not any individuals who may be “at fault” except in extreme circumstances. Many of these practices operate under the owner’s own name and because a reportable breach or settlement becomes part of the public record, a HIPAA issue can attach to an owner’s name well beyond the incident itself. This is not true for every practice, but the underlying accountability works the same way regardless: the owner is the ultimate level where accountability lives.
Many practice owners decide to delegate responsibilities like HIPAA compliance, which is perfectly reasonable, but maintaining oversight is advised considering what is ultimately at stake. At a minimum, that means checking in with whoever manages the details to ask for the date of the last risk analysis, the status of staff training, and any open items from a prior review.
What Noncompliance Actually Costs
Penalties for HIPAA violations scale with the nature of the violation and the practice’s compliance history. Regulators also look at a practice’s financial position when setting the amount: the fine is not designed to bankrupt a practice, but it is designed to hurt, and a small practice’s thin margins and limited cash reserves make that pain land harder than it would for a larger system facing the same underlying violation.
The fine, though, is usually the smallest piece of what an actual breach costs. Figuring out what happened and how far it spread often means bringing in forensic help. Then comes recovery, patient notification, and the reputational fallout of lost patients and the revenue that goes with them. A larger breach can also draw attention from law firms that monitor the public breach records and file class action lawsuits, adding even more costs.
None of this is fully avoidable. A strong program lowers the risk of a breach, but nothing eliminates that risk entirely. What a practice has the most control over is the fine itself. A practice that can show a documented, good-faith compliance effort is positioned to avoid at least that piece of the cost.
Understanding What the Practice Is Actually Obligated to Do
A HIPAA compliance program exists because a practice handles patient information, and federal law sets specific expectations for how that information gets protected, used, and disclosed. Those expectations come from three related rules: the HIPAA Privacy Rule, the HIPAA Security Rule, and the HIPAA Breach Notification Rule. Together they cover who can access patient information, how it needs to be secured, and what happens if it is exposed.
The underlying requirements do not shrink for a smaller practice. A solo practitioner and a ten-provider group face the same rules, but applying them gets more complex as a practice grows, with more systems, more staff, and more vendors to account for. Size affects capacity and complexity. It does not affect what is actually required.
Where the Program Starts
Every compliance program starts with an honest look at where patient data actually exists in the practice and what protects it today. HIPAA has a name for that ongoing process: a Security Risk Analysis. It is documented work, not a one-time form to fill out, that establishes the practice’s baseline risk and tracks progress reducing it over time. An owner should be able to confirm when it was last done, who did it, and what remediation items came out of it. An analysis older than a year, or one that has never accounted for a new system the practice adopted, is an open gap worth asking about directly.
Confirming Policies and Training Are in Place
There are several other critical elements to a compliance program beyond the risk analysis. A policy library, built in part from what the risk analysis reveals, spells out how the practice actually operates and what staff are expected to do in specific situations. A training program then uses those same policies, along with everyday security topics, to reinforce that expected behavior. Together, these are what prevent the kind of human-error breach that is the most common type a practice faces. Most owners delegate or outsource training, and often policy development as well, but the policies still need to reflect how the practice actually operates and not a one-size-fits-all template.
While training gives staff the instruction to follow proper procedure, a sanctions policy is what backs that up. This is a documented statement of what happens when someone does not follow policy, with consequences ranging from a warning to termination depending on the severity of the violation. Having this in writing, and applying it consistently, gives an owner clear grounds to act when someone falls short, and it also shows an investigator that the practice’s rules were actually being enforced.
An Easy Gap to Miss: Vendor Agreements
A practice’s list of vendors tends to grow quietly over time, often without a matching update to its agreements with them. Billing services, scheduling platforms, cloud storage providers, and IT support contractors typically all need a signed HIPAA Business Associate Agreement (BAA) before they can access patient data. This is an area of compliance that rarely comes up in daily operations, so an owner who has not personally checked the vendor list against the practice’s signed BAAs can easily be unaware of a gap that has existed for years, sometimes until an incident forces the review.
This makes vendor oversight one of the larger risk areas for a small practice, for two reasons. First, it is easy to overlook. The practice is usually focused on internal measures and fails to think about these vendors at all. Secondly, these vendors often handle data for many practices at once, which makes them a more likely source of a breach than the practice’s own systems. When a breach does trace back to a vendor, without a BAA the practice still faces serious judgement with the Office for Civil Rights, regardless of where the actual fault lay.
Preparing for an Investigation or Breach
When a breach occurs or a patient files a complaint, documentation, not intention, determines how the investigation resolves. An owner who has maintained oversight of a current, documented program enters that process with evidence the practice acted in good faith. An owner who cannot produce basic documentation faces a much harder path through the same investigation, regardless of how well the practice actually operated day to day.
During an active investigation, the owner typically serves as the practice’s primary point of contact and decision-maker, even when a Privacy Officer or outside counsel manages the technical response. An owner already familiar with the practice’s own compliance documentation responds to the process more effectively than one encountering it for the first time, and avoids the delay of scrambling to locate records that should have been maintained all along.
Staying Current with Regulatory Change
HIPAA requirements change through new rules, updated guidance, and shifting enforcement priorities from the Office for Civil Rights. An owner does not need to track every development personally, but they do need to confirm that whoever manages the practice’s compliance program has a process for identifying relevant changes and applying them, since a policy that reflects an outdated version of a rule is a gap that can sit unnoticed until it matters.
State law adds another layer, and in some ways a harder one to track. There are more states to watch than there are federal agencies, state regulators and courts tend to move faster than federal rulemaking, and many state requirements are stricter than HIPAA’s baseline. Every practice is expected to stay current with both.
Choosing How to Run the Program
A small practice owner generally chooses among three approaches: handling compliance internally with existing staff and generic templates, engaging an outside consultant for periodic review, or adopting dedicated software built specifically to generate and maintain the program. Each carries real tradeoffs in cost, staff time, and how current the program stays between reviews, and the right fit depends heavily on the practice’s specific situation.
The post Small Practice Owners Guide to HIPAA Compliance Programs appeared first on The HIPAA Journal.
 What other features should you consider for your HIPAA compliance solution?
What other features should you consider for your HIPAA compliance solution?
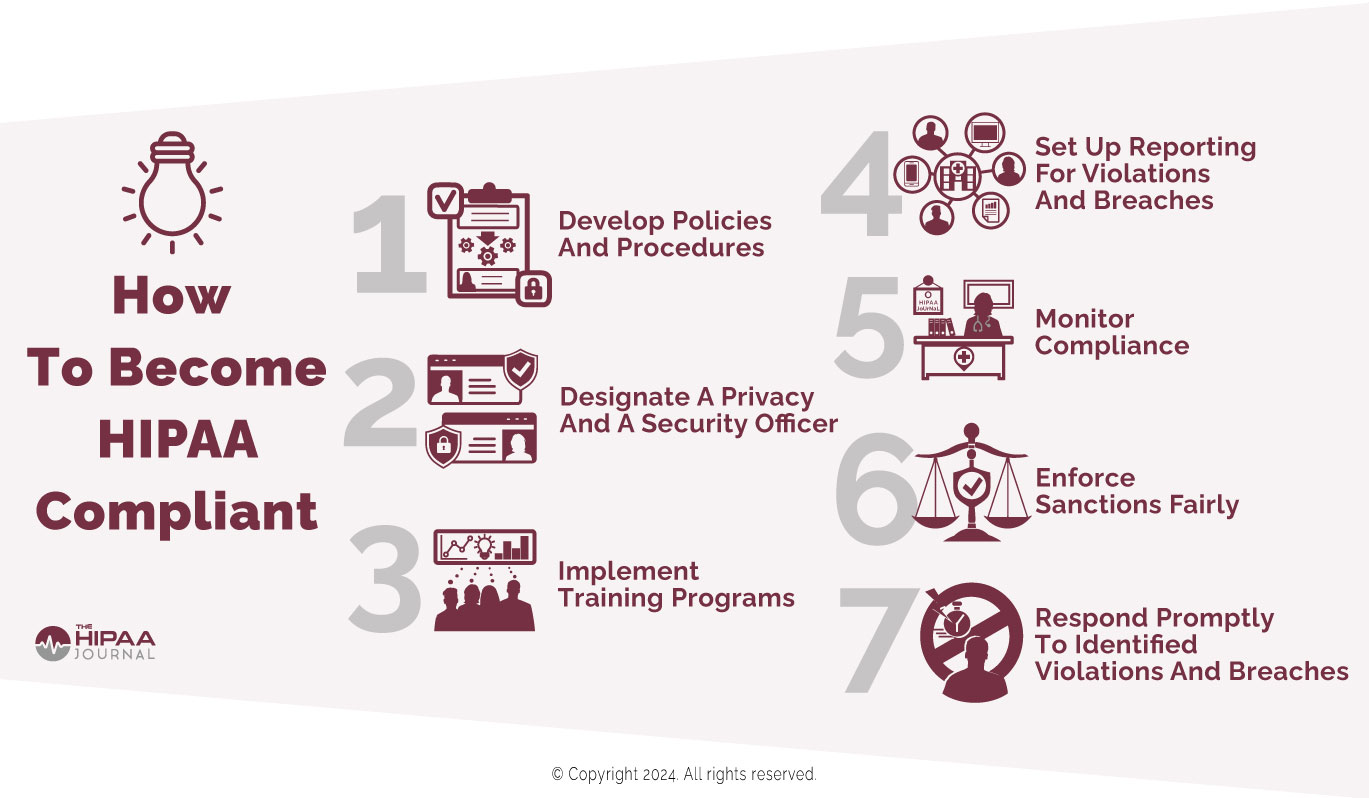
 When considering how to become HIPAA compliant, one of the simplest approaches is to adopt HHS’s “Seven Fundamental Elements of an Effective Compliance Program.” This will help you address compliance challenges identified in a HIPAA risk assessment. It can also be beneficial to take advantage of HIPAA compliance software that is built around The Seven Fundamentals in order to maintain a compliant workplace.
When considering how to become HIPAA compliant, one of the simplest approaches is to adopt HHS’s “Seven Fundamental Elements of an Effective Compliance Program.” This will help you address compliance challenges identified in a HIPAA risk assessment. It can also be beneficial to take advantage of HIPAA compliance software that is built around The Seven Fundamentals in order to maintain a compliant workplace.